Early Signs of COPD: How to Recognize Stage 1 Symptoms
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory condition characterized by reduced airflow and impaired oxygen supply. Simply put, it affects how air moves in and out of the lungs. The first signs of COPD are subtle and often mistaken for aging or low fitness. Detecting the disease early is crucial: with timely care, patients have the chance to slow its progression and keep leading an active, fulfilling life.
Understanding the Condition Before Early COPD Symptoms Become Obvious
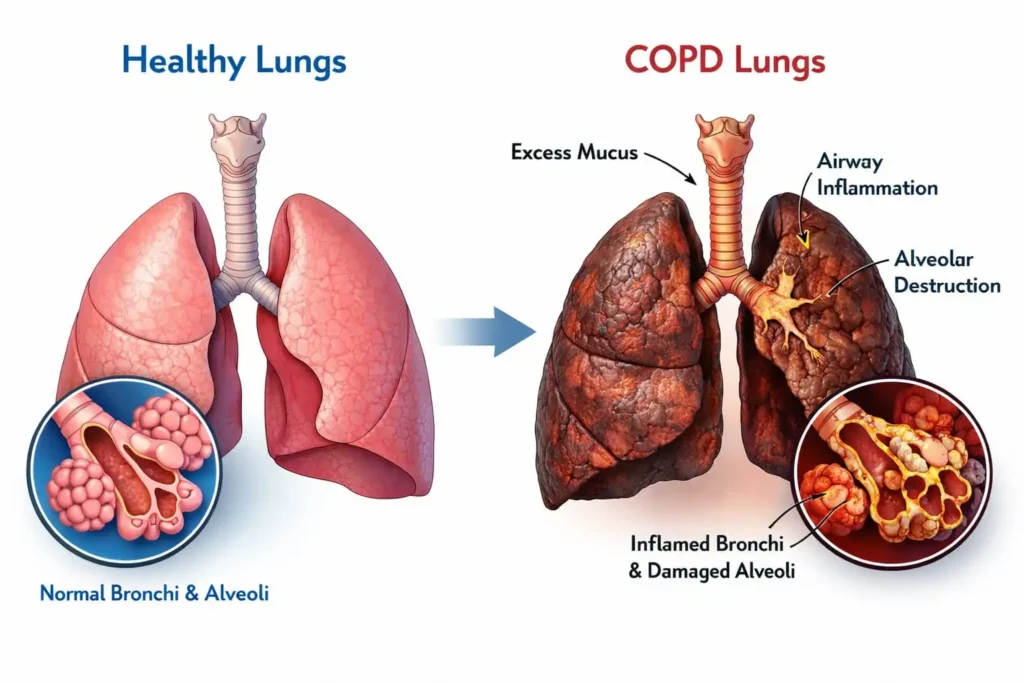
What is COPD? It is a progressive inflammatory lung disease. The condition develops gradually and involves both airway narrowing and damage to the alveoli—the tiny air sacs responsible for oxygen exchange. Over time, the lungs lose elasticity, making breathing increasingly difficult and causing symptoms such as shortness of breath, fatigue, and chronic cough with sputum.
An important characteristic of this condition is the difference between physical airway damage and how patients perceive their symptoms. Inflammation and narrowing of the airways can begin long before noticeable discomfort occurs. This explains why the first symptoms of COPD may feel subtle, despite measurable changes in lung function already taking place.
First Signs of COPD: Why Early Detection Matters for Long-Term Lung Function
In the early stages of COPD, chronic inflammation affects the small airways (particularly the terminal bronchioles), leading to structural changes and narrowing. At the same time, destruction of lung tissue reduces elastic recoil. The combined effect of these processes results in airflow limitation, which becomes evident during pulmonary function testing.
Research shows that the rate of decline in lung function in the early stages largely determines the subsequent course of the disease, the risk of exacerbations, and the development of respiratory failure. Early diagnosis changes treatment strategies, focusing on risk factor modification, environmental exposures, and pharmacotherapy.
Furthermore, patients diagnosed early with COPD tend to have a better quality of life and maintain higher levels of physical activity over the long term.
Recognizing the early signs of COPD is not just about early diagnosis—it is a real opportunity to influence the natural course of the disease.
The Earliest Warning Signs: What Are the Early Symptoms of COPD?
The first signs of COPD are often mild and nonspecific, making them easy to dismiss. Yet they reflect structural and functional airway changes.
Chronic Mucus Production: More Than a Morning Habit
Chronic mucus production may be one of the early signs of COPD and is closely linked to goblet cell hyperplasia, a process in which the number of mucus-secreting cells in the airway lining increases. This cellular adaptation develops in response to persistent irritation, commonly from tobacco smoke or industrial aerosols.
Daily mucus production, caused by chronic bronchial irritation, differs from an occasional morning cough and indicates a pathological process, often associated with thickened airway walls and early airflow limitation.
Physical Fatigue and Its Connection to Reduced Oxygen Efficiency
Unexplained fatigue may be a first sign of COPD. Even small ventilation changes can impair gas exchange, reducing oxygen delivery to muscles and organs, causing people to feel tired more quickly. Systemic chronic inflammation further affects metabolism and energy levels, often before breathlessness becomes obvious. These changes may emerge as subtle, intermittent symptoms during daily activity.
Recurrent Chest Infections as an Early Red Flag
Frequent respiratory infections may be an early sign of COPD.
Impaired mucociliary clearance reduces the lungs’ ability to remove mucus and pathogens, increasing vulnerability to respiratory infections. This, in turn, leads to increased susceptibility to pathogens.
Frequent episodes of bronchitis or “prolonged colds” may therefore reflect early structural airway changes characteristic of the early stages of COPD.
Clinical Perspective: What Defines Stage 1 (Mild) COPD?
COPD clinical classification is based on the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria. The diagnosis is established when persistent airflow limitation is confirmed by spirometry, while disease stage is defined by the degree of functional impairment.
-
1
Functional criteria (spirometry): Stage 1 COPD is characterized by a post-bronchodilator FEV₁ ≥ 80% of the predicted value in combination with an FEV₁/FVC ratio < 0.70, indicating mild but measurable airflow limitation.
-
2
Clinical presentation: Despite detectable functional changes, patients at this stage may report minimal or nonspecific symptoms, as early physiological alterations can be partially compensated.
-
3
Diagnostic correlation: Radiological, functional, and symptomatic findings may differ. Imaging may show limited structural abnormalities, spirometry can reveal airflow obstruction, and symptoms may remain subtle, which can contribute to delayed recognition of the disease.
The Beginning of Symptoms of COPD. What Causes Early Lung Damage? Smoking and Environmental Triggers
- Cigarette smoke: the primary risk factor, causes chronic airway inflammation and alveolar destruction.
- Air pollution: fine particles and toxic gases increase oxidative stress and damage lung tissue.
- Occupational exposure: prolonged contact with dust, chemicals, and aerosols—promotes early airway obstruction.
- Passive smoking: indirect exposure can trigger inflammation and early COPD changes.
- Synergistic effect of inflammation + toxins: even low-level exposures, when combined with chronic inflammation, can accelerate lung damage.
When Does COPD Really Begin? Age and Risk Factors
Recognizing Early COPD Symptoms in Your 30s and 40s
Although COPD is commonly associated with older age, it may begin much earlier. Structural and inflammatory changes may occur in the 30s or 40s, even without persistent symptoms. These early manifestations are nonspecific—mild breathlessness, increased mucus, or fatigue—leading to misdiagnosis as asthma, recurrent infections, or poor fitness.
Alpha-1 Antitrypsin Deficiency: When do COPD Symptoms Start Unusually Early
Alpha-1 antitrypsin deficiency represents a distinct form of COPD with a distinct underlying cause and a more aggressive disease course. Because this genetic condition limits the lungs’ natural protection against inflammatory damage, structural lung changes tend to develop and progress more rapidly.
As a result, individuals with this diagnosis may experience significant respiratory impairment at a younger age and by mid-adulthood can already have a disease burden comparable to much older patients with smoking-related COPD.
Testing is recommended for young patients with early COPD signs, particularly if they have little or no smoking history or a family history of lung disease. Identifying underlying risk factors allows for earlier monitoring and preventive strategies.
Missing Early Signs of COPD: Why COPD Is Often Diagnosed Too Late
COPD often begins quietly—but early recognition can change the course of the disease.
Mistaking breathlessness for aging or low fitness
Mild shortness of breath or a chronic cough is often mistaken for aging or low fitness. Patients frequently delay check-ups and avoid mentioning symptoms to clinicians. This behavior contributes to late recognition, reducing opportunities for early intervention.
How Delayed Recognition of Early COPD Symptoms Worsens Long-Term Outcomes
When early signs are overlooked, COPD may progress to irreversible structural damage: alveoli lose elasticity, the bronchi remodel, and the potential for functional recovery becomes increasingly limited. Late diagnosis accelerates progression: FEV₁ declines faster, exacerbations increase, and complications are more frequent. Early detection is crucial to slowing progression and maintaining quality of life.
Get a free online consultation
If you recognize your symptoms in this article, you can book a free online consultation with regenerative medicine specialists to find out if your condition can benefit from supportive stem cell treatment.

Medical Advisor, Swiss Medica doctor
The Role of Chronic Inflammation in COPD Progression
Chronic inflammation is a central mechanism driving the development and progression of COPD. Acute inflammatory responses go away after an injury, but in COPD, inflammation stays active over time, causing tissue damage and a decline in function.
This process involves complex interactions between immune cells, oxidative stress, and structural changes within the airways. Understanding these mechanisms helps explain why the disease can advance even when symptoms appear mild or risk factors have been removed.
-
1
Persistent immune activation: neutrophils, macrophages, and T-lymphocytes maintain chronic airway inflammation, damaging tissue.
-
2
Oxidative stress: free radicals from toxins and immune cells amplify inflammation, impairing lung function.
-
3
Structural remodeling: thickened bronchial walls, fibrosis, and loss of elasticity reduce airway patency and develop before noticeable symptoms.
-
4
Persistence after smoking cessation: epigenetic changes (lasting changes in how genes function caused by years of smoking), immune dysregulation, and accumulated structural damage sustain inflammation.
Targeting inflammation early, including via regenerative therapies, is key to slowing disease progression.
Can Lung Damage Be Reversed? A Medical Reality Check
The question of reversibility is one of the most common concerns among patients. To answer it honestly, it is important to distinguish between managing symptoms and restoring damaged lung tissue.
Conventional medicine: symptom control vs. regeneration
Conventional therapy focuses on symptom management and slowing progression, rather than on regeneration of lung tissue.
- Bronchodilators, medications that widen the airways, form the backbone of symptomatic treatment. They reduce bronchial smooth muscle spasm, improve ventilation, and ease breathlessness. However, their effects are only functional.
- Corticosteroids are sometimes used to suppress inflammation, mostly in patients with frequent exacerbations. They can dampen immune activity but do not regenerate lung tissue.
- Pulmonary rehabilitation improves physical endurance, breathing mechanics, and overall well-being. Nevertheless, its benefits are also functional and adaptive: rehabilitation helps the body make better use of remaining resources but does not trigger tissue repair processes.
COPD Medications and Treatment Options: Managing Symptoms and Improving Quality of Life
Unfortunately, COPD cannot be completely cured, but there are several treatment options that can help manage symptoms and slow disease progression. This article provides a detailed overview of these approaches, outlining their potential benefits and limitations.
Lung tissue repair at the cellular level: what science says
Recent research suggests that the lungs can repair themselves, but only to a limited extent. Even after harmful exposures are removed, the body often adapts to the damage rather than restoring lost structures, which explains the progressive nature of COPD.
A key role in the lungs’ repair response is played by specialized cells known as alveolar type II cells. These cells help rebuild the damaged lining of the air sacs by activating tightly regulated signaling pathways that coordinate tissue repair and regeneration.
Although the lungs’ natural repair system cannot simply be “replaced” or implanted, certain cell-based therapies may help stimulate the body’s own repair processes, even when long-term damage is present. Stem cells are a major focus because they can create a supportive microenvironment and stimulate endogenous AEC2s to help repair lung tissue.
This approach is not considered an immediate “cure” for the lungs but offers the opportunity to slow COPD progression and support natural regeneration. In the following sections, we will discuss how stem cells can positively influence lung repair.
COPD Medications and Treatment Options: Managing Symptoms and Improving Quality of Life
Mesenchymal stem cells (MSCs) are known for their ability to regulate immune responses, which makes them of interest in research on stem cell therapy for COPD. Explore the possibilities of stem cell therapy in our dedicated article.
Why Stage 1 COPD Represents a Critical Treatment Window
In stage 1, the lungs largely retain structure and elasticity, with minimal fibrosis. Early intervention improves therapy response, preserves function, and enhances the effectiveness of regenerative strategies targeting inflammation and endogenous stem-like cells.
Stem Cell Therapy for COPD: Current Scientific Evidence
- MSC therapy has shown safety and improvements in quality-of-life measures, reduced exacerbations, and enhanced microcirculation, though FEV₁ changes are often minimal. Evidence supports symptom stabilization, slower functional decline, and reduced inflammation.
- A broader systematic review of multiple small trials found that stem cell-based therapies may improve some functional outcomes, such as the distance walked in six minutes, but the evidence for consistent improvements in lung function or reductions in hospitalization risk is not yet definitive.
- Treated patients showed improvements in lung function, exercise tolerance, and quality of life, suggesting that potential stem cell treatment for COPD may help address structural damage.
How mesenchymal stem cells (MSCs) modulate airway inflammation
Mesenchymal stem cells (MSCs) are known for their ability to regulate immune responses, which makes stem cell therapy for COPD of interest in research.
By calming excessive inflammatory activity, MSCs protect lung tissue and support the lungs’ own repair cells, helping them function more effectively. They also promote blood flow and tissue repair by releasing growth factors that improve oxygen delivery and stimulate alveolar cell proliferation. Together, these effects can contribute to gradual structural and functional improvements in the lungs.
The Swiss Medica Approach to Early-Stage Lung Disease
In many highly regulated healthcare systems, stem cell therapies remain limited to clinical trials, which can make them costly or difficult to access.
Swiss Medica, based in Serbia, offers patients a more accessible treatment pathway. With multidisciplinary teams, integrated laboratory capabilities, and personalized care protocols, the clinic provides comprehensive regenerative treatment within a regulated European framework.
- Specialized Expertise: A multidisciplinary team of specialists collaborates to evaluate each patient’s individual needs.
- Personalized Care: Treatment plans address lung disease, overall health, and recovery needs.
- Integrated Laboratory: On-site lab ensures safe, precise cell processing.
- 24/7 Medical Supervision: Patients are monitored around the clock by qualified medical staff at the Swiss Medica treatment facility to ensure safety and timely clinical support.
Swiss Medica’s protocol
Our stem cell clinic follows an approved and safety-focused treatment protocol:
- Patient selection: early-stage COPD screening, medical review, diagnostics.
- Safety framework: on-site lab ensures cell viability and sterility.
- Individualized treatment planning: therapy tailored to lung condition, comorbidities, and goals.
- Integrated approach: combines stem cells with supportive and rehabilitative therapies.
- Follow-up: monitoring lung function and adjusting rehabilitation to maximize outcomes.
Expected Outcomes of Stem Cell Therapy for COPD
Stem cell therapy in COPD aims to modulate inflammation and support lung tissue rather than provide immediate restoration or a complete “cure.”
An important goal of this section is to help patients form realistic expectations and understand that outcomes depend on disease stage, individual characteristics, and adherence to the treatment protocol.
- Reduction in chronic inflammation: MSCs lower pro-inflammatory activity and support alveolar repair.
- Potential improvement in exercise tolerance may be linked to reduced inflammation and enhanced microcirculation.
- Slowing of functional decline: stem cell therapy can help stabilize symptoms and slow the progression of the disease.
- The timeframe is gradual: effects may appear over weeks to months; combination with rehabilitation enhances benefits.
Patient Case Review at Swiss Medica
In this video, a patient shares his personal experience with stem cell therapy for COPD, describing perceived improvements in daily functioning and overall quality of life.
While individual responses to treatment can vary, this testimonial reflects how some patients report symptomatic relief following stem cell therapy.

You can find more reviews on our YouTube channel.
The stem cell therapy success rate is not uniform and depends on several key factors, including the stage of the disease, the patient’s overall health status, and individual biological response to treatment.
Living With Stage 1 COPD: Practical Lifestyle Adjustments
Even in early-stage COPD, a healthy lifestyle plays a key role in slowing disease progression and supporting lung function.
- Smoking Cessation. Quitting smoking is the most effective way to protect the lungs from further damage. Any effort to stop smoking significantly reduces disease progression and chronic inflammation.
- Physical Activity. Regular moderate exercise improves breathing mechanics, increases endurance, and supports cardiovascular health. Pulmonary rehabilitation programs, including breathing exercises and aerobic activity, are especially beneficial.
- Nutrition. A balanced diet rich in protein, antioxidants, and vitamins helps maintain immunity and preserve muscle mass, which is important for staying active with COPD.
- Infection Prevention. Patients with Stage 1 COPD should stay up to date on flu and pneumococcal vaccines, avoid contact with people with respiratory infections, and practice good hygiene to reduce the risk of exacerbations and maintain stable lung function.
How to Start an Evaluation for Stem Cell Therapy for COPD at Swiss Medica
If you are considering stem cell therapy for COPD, the first step is a free, no-obligation consultation with the Swiss Medica medical team.
During this evaluation, you can share your medical history, recent lung function tests (including FEV₁ and imaging results), current medications, and any past treatments. The team will review your records and discuss whether regenerative therapy may be appropriate for your condition.
If you are ready to explore your options, you can book a consultation and speak directly with a medical specialist, who will guide you through the next steps and help you understand the potential benefits and realistic outcomes of stem cell therapy for COPD.
Contact us
Book a consultation now and speak directly with a medical specialist.
Medical Advisor, Swiss Medica doctor
Frequently Asked Questions
1. What are the symptoms of COPD in stage 1 that are most often overlooked?
In early-stage COPD, many symptoms go unnoticed or are attributed to aging or low physical activity. The most common sign is mild shortness of breath during exertion, chronic cough, or increased mucus production. Patients may dismiss these as “normal” for their lifestyle. Early recognition is important, as timely diagnosis and intervention can slow disease progression and help maintain lung function.
2. What are usually the first symptoms of COPD?
The earliest symptoms typically include mild exertional shortness of breath, chronic cough, and increased mucus. These signs are usually subtle and develop gradually, so many people ignore them. Early symptoms may vary depending on factors like smoking, age, and environmental exposures. Monitoring changes in breathing and consulting a doctor at the first warning signs is crucial for early diagnosis and lung support.
3. Are the beginning symptoms of COPD always noticeable?
Early COPD symptoms are not always noticeable. Structural and inflammatory changes in the airways can develop with little or no discomfort. Many people unconsciously adapt by reducing activity or changing breathing patterns, which can mask airflow limitation. As a result, COPD may progress silently for years, highlighting the importance of risk-based screening and objective lung function tests.
4. When should someone with early signs of COPD see a doctor?
If you notice persistent mild shortness of breath, chronic cough, or increased mucus, even if mild, you should see a doctor. Early lung function assessment allows timely treatment, slows disease progression, and supports breathing capacity. It is especially important if risk factors are present, such as smoking, occupational dust or pollution exposure, or recurrent respiratory infections.
5. Can stem cell therapy help improve early COPD symptoms?
Stem cell therapy in early-stage COPD may reduce airway inflammation and support lung function by creating a more favorable environment for endogenous regenerative cells. Some patients notice improved exercise tolerance and fewer exacerbations. However, therapy does not cure the disease and requires a comprehensive approach with medical supervision. Effects of stem cell therapy appear gradually, depending on disease stage, lung condition, and individual response.
List of References:
Wang, D., Liu, H., Bai, S., Zheng, X., & Zhao, L. (2025). The PAR6B-PRKCI-PAR3 complex influences alveolar regeneration in patients with the emphysema subtype of chronic obstructive pulmonary disease. Stem Cell Research & Therapy, 16, 97. (SpringerLink)
Zhu, Y., Sun, Z., Han, S., et al. (2020). Allogeneic umbilical cord-derived mesenchymal stem cell transplantation for treating chronic obstructive pulmonary disease: a pilot clinical study. Stem Cell Research & Therapy. (Springer)
Liu, X., Zhou, M., Xu, P., et al. (2022). Stem Cell-Based Regenerative Therapy and Derived Products in COPD: A Systematic Review and Meta-Analysis. Journal of COPD, Clinical and Translational Research, PMC9180461. Retrieved from (PMC)
Craig, M. (2023, September 12). Stem cells can be used to repair damaged lung tissue in COPD patients. News-Medical.net. Retrieved from (news-medical.net)
Xu J., Zeng Q., Li S., Su Q. and Fan H. (2024). Inflammation mechanism and research progress of COPD. Retrieved from (PMC)
Wang Y., Meng Z., Liu M., Zhou Y., Chen D., Zhao Y., Zhang T., Zhong N., Li S., Zuo W., et al. (2024). Autologous transplantation of P63⁺ lung progenitor cells for chronic obstructive pulmonary disease therapy. Science Translational Medicine, 16(734): eadi3360.РМС
Medical Advisor, Swiss Medica doctor